
Eyelid Tumours
In recent years, the incidence of eyelid skin cancer has escalated considerably due to the effects of excessive sun exposure in a population previously unaware of its harmful nature.
Effective diagnosis and treatment are crucial since even small tumours can destroy the delicate lid structure necessary for maintaining the health of the eye.
Basal Cell Carcinoma
Eyelid cancers may present in assorted forms, including as areas of elevation, depression, redness, scaliness, or dark or light discoloration.
Some eyelid tumours grow quickly, while others may take several years to reach noticeable size.
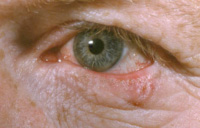
Not all are elevated. Any sore that refuses to heal is suspect.The most common eyelid cancer is basal cell carcinoma, which accounts for more than 90% of cancers in this area.
Typically, it appears nodular (Image 2) and well-localized, but less defined flat or even depressed forms can be more invasive.
While it is unusual for basal cell carcinoma to spread widely through the blood stream, it can cause considerable destruction of eyelid structure, function, and appearance by direct spread.
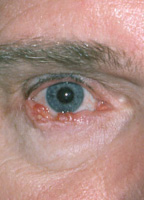
Squamous Cell Carcinoma

Squamous cell carcinoma, the second most common eyelid malignancy, is more aggressive and dangerous than basal cell carcinoma and may spread to local lymph nodes as well as throughout the body.
Less Common Eyelid Cancers
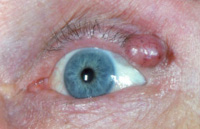
Other eyelid cancers may be much more aggressive and malignant, such as the adenocarcinoma shown here. Such tumours may spread widely and prove fatal.
Any suspicious lesion should be removed immediately and examined under the microscope to determine whether it is benign or malignant.
Biopsy is a quick and easy procedure. Once a diagnosis has been made, complete removal of eyelid cancer is the primary goal of treatment. Burning, freezing, or simply scraping the skin are not recommended over surgery since there is no way to assure that the lesion has been fully removed.
The method of surgical reconstruction is dictated by the size and location of the resulting defect after the cancer has been excised. When applied properly, modern techniques allow for the recreation of a near-normal appearing and functioning eyelid.